ProFee vs Facility Billing & Coding: The Essential Guide

Understanding Professional (ProFee) vs. Institutional (Facility) Billing and Coding
One concept that frequently confuses new medical coders and billers is the difference between professional (ProFee) and institutional (facility) billing and coding. Mastering both is essential to becoming a well-rounded professional in this field.
Professional (ProFee) Coding and Billing
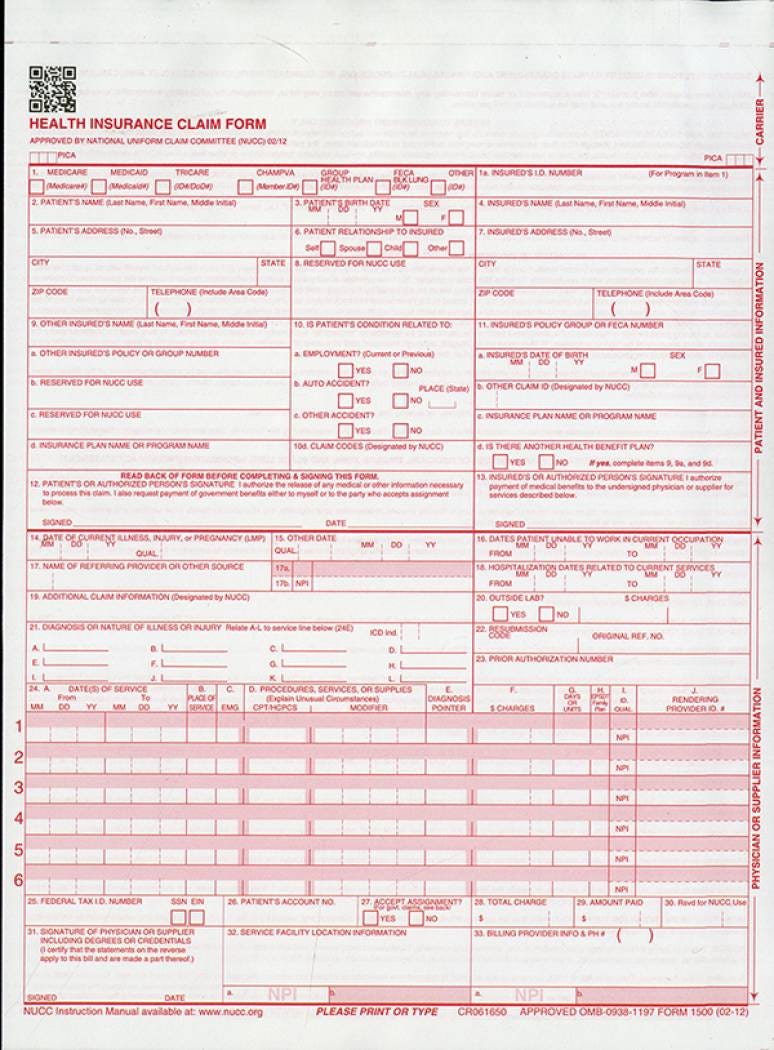
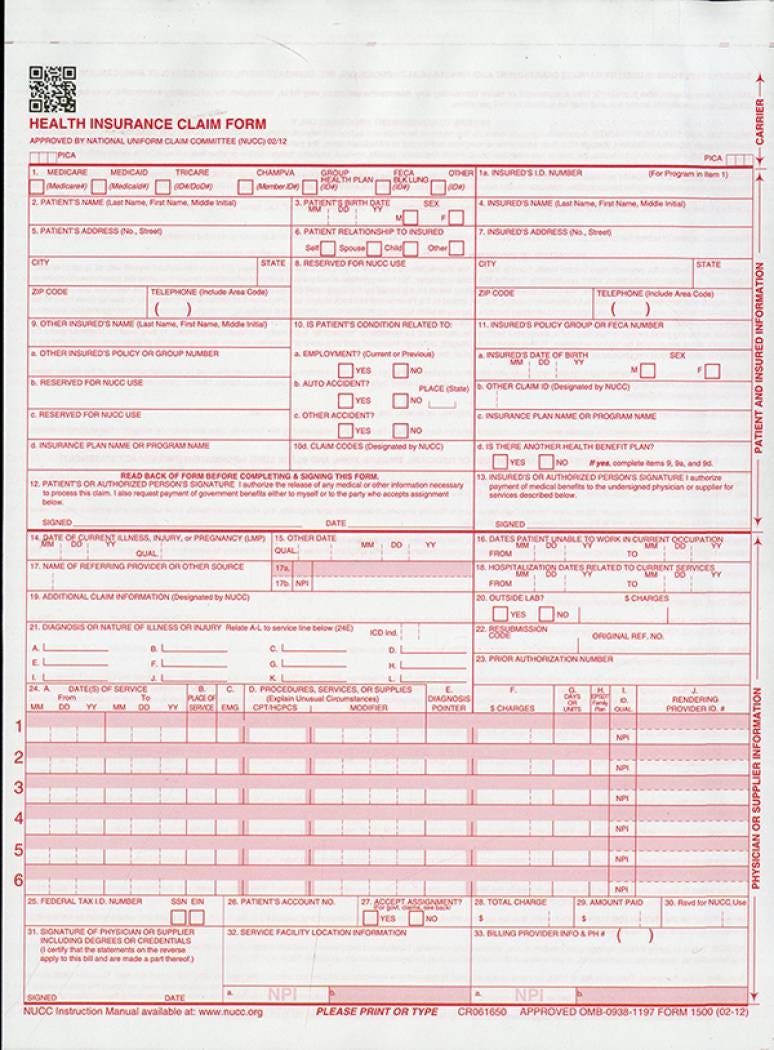
Professional coding focuses on the services provided by individual healthcare providers—physicians, nurse practitioners, physician assistants, and others. These claims are submitted on the CMS-1500 claim form (also known as the professional claim form).
Payment Models for Providers:
Fee-for-Service (FFS): The most common model. Providers are paid for each service, procedure, visit, or test. Each CPT/HCPCS code is assigned Relative Value Units (RVUs), which consist of three components:
Work RVU + Practice Expense (PE) RVU + Malpractice (MP) RVU.
These are multiplied by a conversion factor and adjusted by Geographic Practice Cost Indices (GPCIs) to determine payment. CMS publishes the Physician Fee Schedule (PFS); other payers may adopt it or negotiate their own rates.Value-Based Care: Reimbursement is tied to quality, outcomes, cost efficiency, and performance metrics rather than volume alone. Providers may receive bonuses or face penalties. Payments are often bundled for an entire episode of care.
Capitation: A fixed payment per patient per period (usually monthly), regardless of services rendered. This gives practices predictable revenue but shifts risk to the provider group for managing patient care efficiently.
Hybrid/Salary Models: Many physicians participate in combinations of the above or receive base salaries with productivity incentives.
Below is an example of a CMS-1500 claim form
Institutional (Facility) Coding and Billing
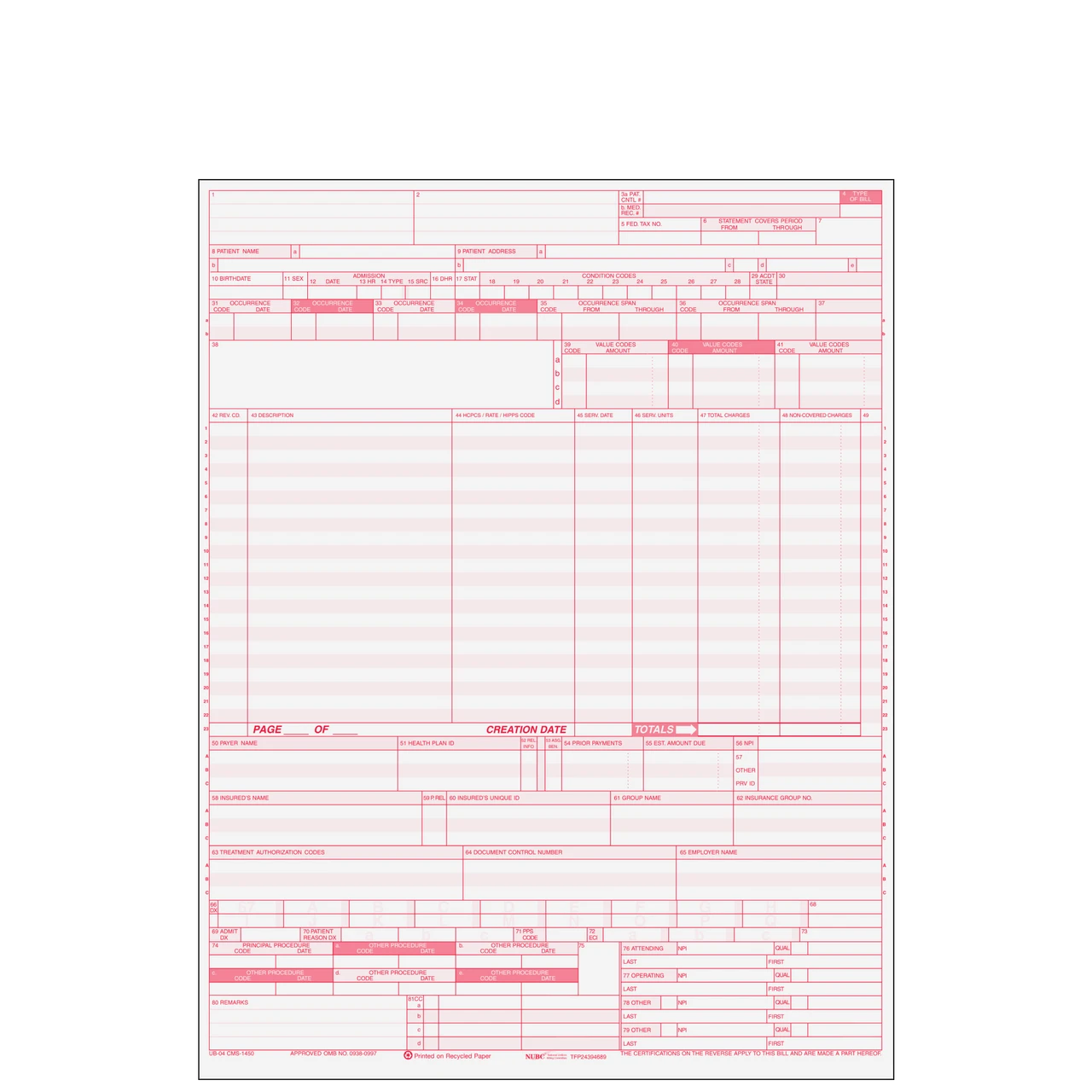
Facility coding reimburses the healthcare organization (hospital, clinic, etc.) for overhead resources such as supplies, medications, room time, nursing staff, equipment, and facility operations. These claims are submitted on the UB-04 form (institutional claim form).
Payment Models for Facilities:
Outpatient Prospective Payment System (OPPS): Medicare’s primary system for outpatient services. Payments are based on Ambulatory Payment Classifications (APCs), which group similar services and assign set reimbursement rates to applicable CPT/HCPCS codes.
Inpatient Prospective Payment System (IPPS): Medicare’s model for inpatient hospital stays. Hospitals receive a fixed payment per discharge based on the patient’s Medicare Severity Diagnosis-Related Group (MS-DRG), which accounts for diagnosis, procedures, severity of illness, and expected resource use.
Per Diem: A fixed daily rate, commonly used for inpatient psychiatric, rehabilitation, or long-term care stays.
Cost-Based Reimbursement: Primarily for Critical Access Hospitals (CAHs). Medicare pays 101% of reasonable allowable costs. This can apply to inpatient, outpatient, and swing-bed services.
Facilities may also participate in capitation, fee-for-service, value-based arrangements, or other specialized models.
Below is an example of the UB04 Claim Form
Code Selection Differences
The code sets you use depend on whether you’re coding for the provider or the facility:
Professional Coding: Primarily uses the CPT codebook (maintained by the American Medical Association) for procedures and Evaluation & Management (E/M) services. You’ll also use ICD-10-CM (maintained by NCHS/CDC, with AMA involvement in guidelines) for diagnoses. Focus is on the provider’s medical decision-making, time, and work.
Facility Coding:
Outpatient: CPT, HCPCS Level II, and ICD-10-CM.
Inpatient: ICD-10-CM (diagnoses) + ICD-10-PCS (procedures).
HCPCS Level II codes (maintained by CMS) are especially important for facility billing of supplies, drugs, and certain services. Medicare often requires them in place of certain CPT codes for facilities, though many commercial payers still prefer CPT. Always check payer-specific guidelines.
Modifier Usage
Modifiers can differ significantly between professional and facility coding:
Primarily Professional Modifiers:
22 – Increased Procedural Services
Global Surgery Modifiers: 24, 57, 58, 78, 79
51 – Multiple Procedures
53 – Discontinued Procedure
54/55 – Surgical Care Only / Postoperative Management Only
Primarily Facility Modifiers (Outpatient):
52 – Reduced Services
73 – Discontinued Outpatient Procedure Prior to Anesthesia Administration
74 – Discontinued Outpatient Procedure After Anesthesia Administration